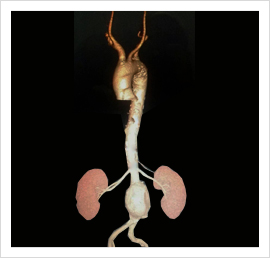
Abdominal Aortic Aneurysms
- An AAA is an increase in aortic diameter by greater than 50% of normal
- Usually regarded as aortic diameter of greater than 3 cm diameter
- More prevalent in elderly men
- Male : female ratio is 4:1
- Risk factors - hypertension, peripheral vascular disease, family history
- Accounts for 2% male deaths above the age of 55 years
- 3000 elective and 1,500 emergency operations in Maharashtra each year
- Mortality of emergency operation is greater than 50%
- Mortality of elective surgery is less than 5%
- Selection of patients for operation depends on risk of operation vs. risk of rupture
Natural history
- AAA diameter expands exponentially at approximately 10% / year
- Risk of rupture increases as aneurysm expands
-
5 year risk of rupture:
- 5.0 - 5.9 cm = 25%
- 6.0 - 6.9 cm = 35%
- More than 7 cm = 75%
Overall only 15% aneurysms ever rupture
85% of patients with a AAA die from an unrelated cause
Screening
- AAA are suitable for screening as elective operation of asymptomatic aneurysms can reduce mortality associated with rupture
- Who should be screened?
- Probably males over 65 years - especially hypertensives
- Single US at 65 years reduces death from ruptured AAA by 70% in screened population
- Patients with small aneurysms should undergo regular surveillance
- Repeated ultrasound every 6 months
Clinical features
- 75% are asymptomatic
- Possible symptoms include
- Epigastric pain
- Back pain
- Malaise and weight loss (with inflammatory aneurysms)
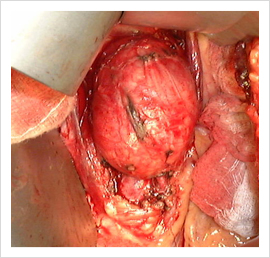
- Rupture presents with
- Sudden onset abdominal pain
- Hypovolaemic shock
- Pulsatile epigastric mass
- Rare presentations include
- Distal embolic features
- Aorto-caval fistula
- Primary aorto-intestinal fistula
Indication for operation
- Rupture
- Symptomatic aneurysm
- Rapid expansion
- Asymptomatic > 6 cm - exact lower limit controversial
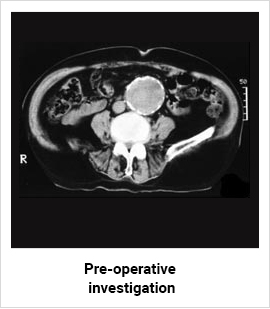
Pre-operative investigation
- Need to determine
- Extent of aneurysm
- Fitness for operation
- Ultrasound, CT Scan
- Determines - aneurysm size, relation to renal arteries, involvement of iliac vessels
- Most significant post op morbidity and mortality related to cardiac disease
- If pre-operative symptoms of cardiac disease need cardiological opinion
- May need thallium scan or cardiac catheterisation
- Cardiac revascularisation required in up to 10% patients
Endovascular aneurysm repair
- Introduced into clinical practice with few clinical trials over the past 10 years
- Exact role unclear and medium and late-complications only recently recognised
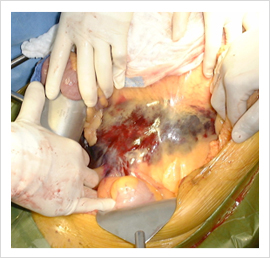
- Morbidity of conventional open aneurysm surgery related to
- Exposure of infra-renal aorta
- Cross clamping of aorta
- Endovascular repair may be associated with
- Reduced physiological stress
- Reduced morbidity
- Reduced mortality
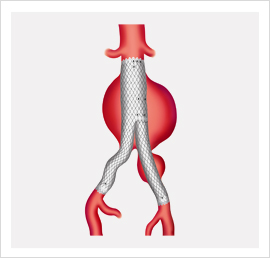
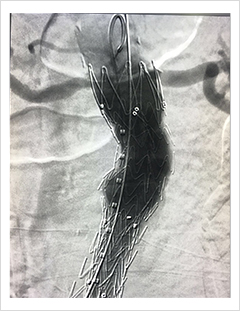
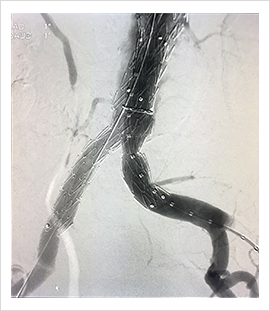
Technique
- Endovascular repair achieved by transfemoral or transiliac placement of prosthetic graft
- Proximal and distal cuffs / stents anchor graft
- Exclude aneurysm from circulation
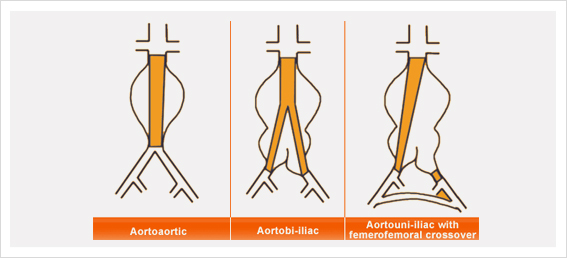
- Three main types of graft
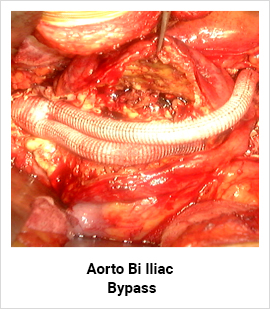
- Aorto-aortic
- Bifurcated aorto-iliac
- Aorto-uniiliac graft with femoro-femoral crossover and contralateral iliac occlusion
- Use of technique depends on aneurysm morphology
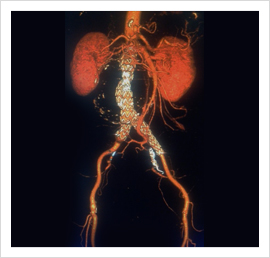
- Aneurysm morphology is best assessed with spiral CT
- Only ~40% of aneurysms suitable for this type of repair
- Aorto-aortic grafts less frequently used due to high complication rate
- Successful stenting associated with reduced aneurysm expansion
- Still has 1% per year risk of aneurysm rupture
Complications
- Graft migration
- Endovascular leak
- Graft kinking
- Graft occlusion
Dr. Pankaj Patel a vascular surgeon has expertise in peripheral vascular diseases, varicose veins and deep vein thrombosis
Open surgery for Aneurysm repair nowadays is done only on young and fit patients.