Intra-arterial thrombolysis
- Arteriogram and catheter advanced into thrombus
- Urokinase 15000u/hr + heparin 250u/hr
- Alternative thrombolytic agents include urokinase or tissue plasminogen activator (TPA)
- Repeat arteriogram at 6 -12 hours
- Advance catheter and continue thrombolysis for 48 hours or until clot lysis
- Success 60-70% but needs careful case selection
- Not suitable if severe neuro-sensory deficit
- Thrombolysis can be accelerated by
- Pulse spray through multiple side hole catheter
- Aspiration thrombectomy - debulking thrombus aspiration
- High dose over shorter time
- Complications
- Mortality of 1-2%
- Bleeding - CVA, retroperitoneal
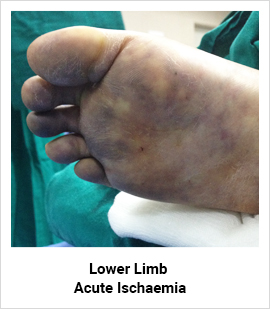
Late presentation. This limb cannot be salvaged and will need amputation
Dr. Pankaj Patel a vascular surgeon has expertise in peripheral vascular diseases, varicose veins and deep vein thrombosis